Hiroshima Nagasaki Survivors
An exces of cancers and leukaemia among survivors
Our knowledge of the risks of cancers due to radiation are largely based on the monitoring of 120,321 irradiated Hiroshima and Nagasaki survivors. This unfortunate population is the main « cohort » available to statistically assess, over a long period of time, the effects of strong irradiations.
Excess of cancers among Hiroshima and Nagasaki survivors
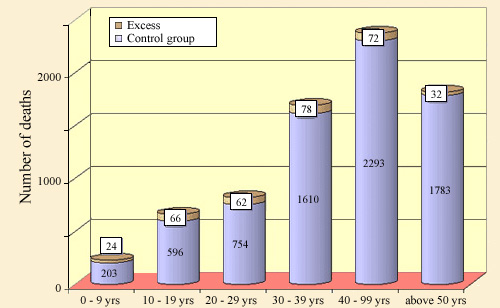
The excess (in orange) of cancer mortalities (others than leukaemia) is obtained from the comparison of irradiated Hiroshima-Nagasaki survivors with a sample of non-exposed population. There is a significant surplus for all ages, 5% on average : 7578 cancer deaths observed against 7244 for the control population, i.e. an excess of 334. The observation period is from 1950 to 1986.
© IRSN
In order to predict the consequences of exposure to medium and low doses of radioactivity, the experts assume that effects are in proportion of received exposures. For example, they would estimate the number of cancers to come within a population given the number of millisieverts received on average per capita. To perform these estimates, they use mainly the results of Hiroshima and Nagasaki studies.
One has to study radiation effects on large samples of population, since it is impossible for medium or low doses to attribute individual deaths to radioactivity. A long period of observation is required. Contrary to a popular belief, even a very high exposure to radiation does not kill quickly. For instance the two victims of the Tokaimura accident survived several months to a fatal dose.
Excess of leukaemia among Hiroshima and Nagasaki survivors
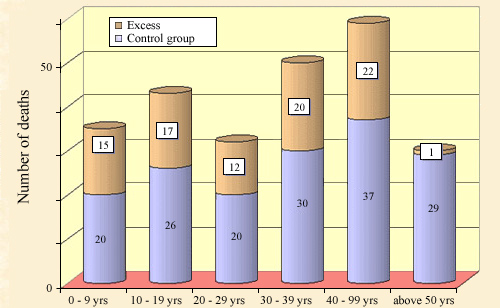
The excess of leukaemia mortality among survivors of Hiroshima and Nagasaki is obtained in a similar way by comparison with a control population. The relative surplus is more pronounced at all ages than for solid cancers. However in total, radiation induced leukaemia were responsible for fewer deaths, 87 compared to 334 deaths than from other cancers.
© IRSN
In the case of the sanitary consequences of the Chernobyl accident, thorough studies have been carried out or are underway. However the hindsight of 25 years remains insufficient. The dispersion of the groups of people the most at risk, such as the Chernobyl liquidators, renders their medical monitoring difficult.
All this means that the data on humans are – fortunately – rare. Nearly sixty years after two atomic bombs were dropped on Hiroshima and Nagasaki, one relies largely on data collected from the residents of these two cities who survived. One must add to these tens of thousands of irradiated people, several hundred workers in the fields of medicine and nuclear industry that were exposed to high doses during accidents.
Since natural radionuclides, such as radium, thorium, uranium, have been used since the early twentieth century, radioprotection experts had a long experience to evaluate their carcinogenic effects. Maurice Tubiana, a pioneer of nuclear medicine in France, cited as interesting cohorts : A) A few thousand workers contaminated in the 1920s for painting radium luminous dials and who were carefully monitored ; B) Patients who had thorotrast injected (a compound containing thorium) as contrast agent in vascular radiology ; C) Uranium miners of the 1950s that breathed a radon-rich air and for whom an increase in lung cancer was found.
Leukaemia and cancer risks
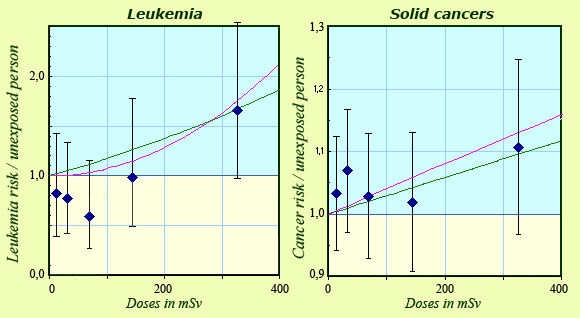
The figure displays, for Hiroshima and Nagasak survivorsi, the ratios of leukaemia or cancers observed to those observed in an unexposed control population. The leukaemia risk differ from other cancers, called solids cancers. It seems that the leukaemia incidence remains low or null up to 200 mSv, then grows sharply while increase would be gradual for solid cancers. Error margins being very important despite the 70,000 cancers concerned. The two models represented here are compatible with the data.
© IN2P3 (Source IRSN/H.Métivier)
Among the Hiroshima and Nagasaki survivors, the number of deaths caused by irradiation is computed by comparison with a control sample of unexposed population. For example, between 1950 and 1990, among the 120,321 survivors 7578 people died of « solid » cancers while the number of expected deaths for the same size sample of unexposed population is 7244. The excess of 334 people (to which 87 leukaemia must be added) is too significant to be due to statistical fluctuation.
This surplus looks modest compared to the 7244 natural cancer occurring in the control sample and the 240 000 direct deaths caused by the explosions. For the irradiated Hiroshima and Nagasaki survivors exposed to doses of several hundred millisieverts, the increase of fatal cancer over forty years amounts only to 4.6% of the cancers occurring from natural causes.
the increase of fatal cancer over forty years amounts only to 4.6% of the cancers occurring from natural causes.
The modesty of these surpluses explains why it is almost impossible to observe the health effects of lower exposures : for an irradiation of one tenth of that received by the Japanese survivors, the excess of cancers would fall to 33 on a total of nearly 7000. Such an excess would be too marginal to be proved.
NEXT : Linear no-threshold model
NB : These surpluses of 334 cancers and 87 leukemias seem small compared to the tens of thousands of victims of the two bombs ! This is because most of the victims were killed because of Shockwave, the fireball, the burns that followed well before radiations may have had their effects.
Other articles on the subject « Radiation Effects »
Deterministic effects
The domain of strong doses and severe, reproducible effects For high doses above a certain thresh[...]
Probabilistic effects
The domain of low and average doses For weak or medium-strength doses, the effects are not as cle[...]
Dose-effects Relationship
Can effects caused by low doses of radiations be predicted ? Even though we are constantly expose[...]
Cumulative Dose
What is the cumulative exposure? We receive an average of 2.5 millisieverts (mSv) per year from n[...]
Dose Rate
Acute and chronic exposures The « effective dose » is not sufficient by itself to characterize on[...]
Linear No-threshold Model
A Precautionary Principle applied to radioactivity … Is it possible to predict the effects [...]
Low doses effects
Do low doses of radiation have any effect? Radioprotection experts commonly refer to doses below [...]
Radiosensitivity
Sensitivity of DNA in living cells to radiation Although we still know little about the effects o[...]
Radioactive Toxicity
A useful indicator but to be used appropriately … The danger presented by a radioactive sub[...]
Dose Factors
What doses when swallowing or inhaling radioactive atoms ? How to evaluate the doses resulting fr[...]