Radio and nuclear therapies: Doses are high but local
Genuine nuclear therapies (brachytherapy, proton therapy, or metabolic therapies) are much less used than the ones based on X-rays or gamma rays. So when talking about doses in this field, it is usually about radiotherapy or teletherapy.
Whatever the origin of the rays, the aim is always to destroy malignant cells while sparing the healthy neighbor tissues as much as possible. Radiotherapists try to focus the rays toward the tumour location. The most significant dose for the patient and the physician is the energy density absorbed in the malignant tissue in question.
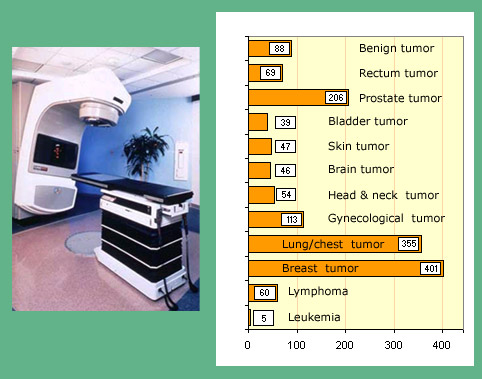
Frequencies of major radiotherapies
Average number of teletherapies per million populations in developed countries.
©IN2P3/Source K.G.Gerber – Unscear 2000
In this context, it is a local irradiation that it is vital to distinguish from a global irradiation. In therapy, the absorbed energy densities are tens of joules per kilogram or grays. These high doses of radiation, bearable as they are local, would be fatal if they were provided to the entire body.
In diagnosis, where doses are low, practicians evaluate the effective dose in order to minimize, as much as possible, the resulting global exposure and therefore the risks. In therapy, the whole body exposure and the effective doses are much more important than during diagnosis. The associated risks are considered as an unavoidable but minor compared to the possibility of curing cancer (philosophy of acceptable risk).
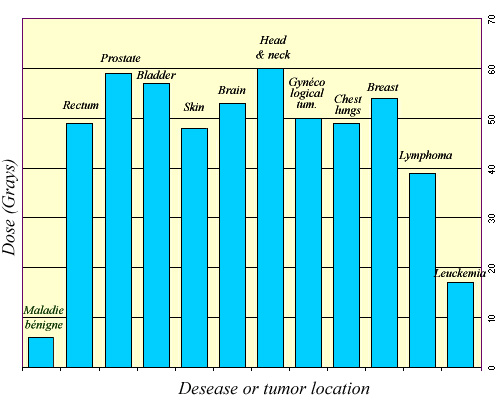
Average doses in radiotherapy
Radiotherapy doses are expressed in grays. These are average because the doses prescribed may vary from one patient to another. The use of gray as a unit instead of the Sievert is necessary because in therapy one considers doses locally delivered to the tumor. Sievert and its sub-multiples are units planned for radiation protection, not for the energy deposited in a tumor for its destruction.
© IN2P3/ Source K.G.Gerber – Unscear 2000
The consideration of a certain accepted risk does not mean that everything must not be done to reduce this risk. The irradiations of healthy tissues are inevitable when a tumor is treated with an external source of radiation, which is the general case. X-rays or gamma go through healthy tissue located in front of the tumor, and those who were not absorbed yet go through tissues located behind the tumor. In modern therapies, a careful collimation of the rays avoids irradiating nearby the tumor. By varying the angle of attack, radiation is concentrated in the tumor while sparing the surroundings. Very sensitive organs should also been spared, which is not always possible or which require to use rays stopping inside the tumor, as protontherapies.
The intensity of irradiation, the degree of risks, requires high precision (higher than 5%) in the monitoring of absorbed doses at various treatment stages. One must continuously control the radiation, which is evaluated from dosimeters measuring radiation and located in sensitive places near the patient.
Other articles on the subject « Expositions in Medicine »
Radiation doses in diagnostics
From simple radiology to PET scans and scintigraphy Scintigraphy scans are by far the most common[...]
Doses (X-Rays, CT scans)
Exposures to radiations in diagnostic radiology The vast majority of diagnoses based on radiation[...]
Doses (nuclear diagnostics)
Nuclear medicine : doses in nuclear diagnostics Nuclear medicine examinations are performed only [...]
Doses in Nuclear therapies
High local doses In nuclear therapy, the doses delivered to tumours amount to few tens of Grays. [...]